We investigated: (a) relationships of self-reported home coastal proximity and coastal visits with self-reported general health; (b) their potential to buffer income-related health inequalities; and (c) the generalizability of these propositions across 15 countries, using a Bayesian approach.
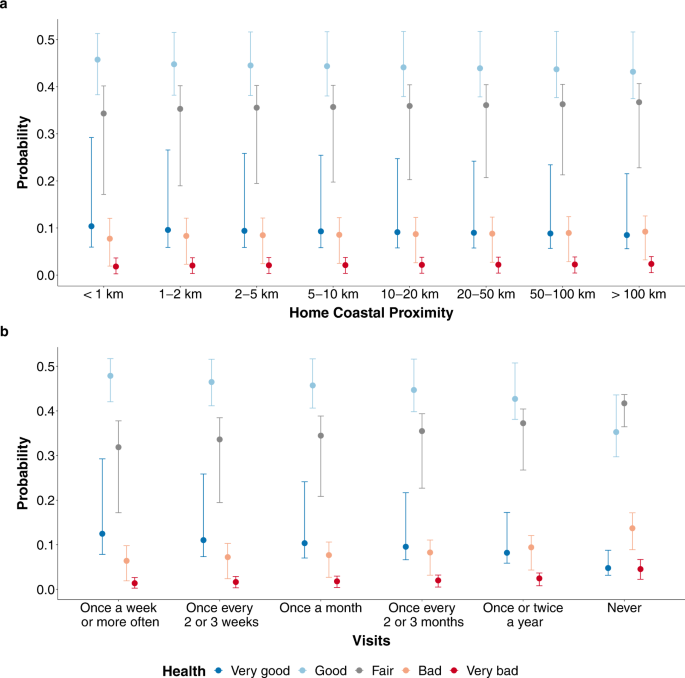
Living nearer to the coast predicts better self-reported health within countries across Europe and Australia, with a similar yet rather small magnitude (Table 1). Importantly, 37.9% of the total improvement in health when living nearer to the coast happens between <1 km and 1–2 km, suggesting that most health benefits arise from living very close to the coast. Smaller changes (6.7–18.2%) occur between the other adjacent distance categories. These findings are consistent with Wheeler et al.3 that, for example, self-reported health is better for those living 20–50 km compared to more than 50 km from the coast. Overall, the coast provides people with a wide range of health-promoting opportunities (e.g., physical activity1,7). Living very close to the coast may make people more likely to take advantage of these opportunities6.
Table 1 Summary of the results. Full size table
Visiting the coast more often also predicts better self-reported health within countries (Table 1). Notably, 53.4% of this total effect happens between visiting ‘once or twice a year’ and visiting ‘never’. This does not necessarily mean that the largest health benefits arise when visiting the coast once a year compared to never visiting it. Rather, we recognize the possibility of reverse causality here, such that individuals who never visit the coast may differ from other groups (e.g., by having a chronic illness), which limits their visit opportunities/mobility. The visits-health relationship varies across countries in terms of magnitude, with the strongest relationship in Ireland and the weakest in Italy, potentially because of high coastal tourism20 and longer travel distances in Italy (percentage of respondents who live >20 km from the coast in Ireland: 34.4% vs. Italy: 57.3%) may limit the value of the coast for locals. Moreover, the coast may be less accessible in Italy compared to other countries due to high coastal privatization21.
Supporting previous single-country studies1,2,3,4,5,6,10,11,22,23,24, the findings strengthen the evidence that living nearer to the coast and visiting it more often are associated with better self-reported health. Access to coastal environments may thus represent a viable and unified route to public health promotion across Europe and Australia.
Besides these direct effects, this study provides very and extremely strong evidence against the ‘buffering’ role of coastal contact on the income-health relationship. Lower household income is more strongly associated with poorer health when living nearer to the coast, thereby potentially reinforcing existing income-related health inequalities. However, we recognize that this effect is very small, and the results are also compatible with a null effect that the income-health relationship is similar regardless of how far individuals live from the coast.
This finding is in direct contrast to previous research that found a ‘buffering’ effect of coastal proximity for both general health, using the same outcome variable as here3, and mental health17. However, it aligns with a previous finding that more green spaces are associated with poorer health in low-income areas, potentially because green spaces in these areas are of poorer quality16. Coastal quality may also explain the current findings. When individuals with lower household incomes live near the coast, they may be more likely to live in areas of poor aesthetic and environmental quality because housing prices in such areas tend to be lower (e.g., water quality and housing prices25).
The current study also finds that lower household income is associated with poorer health regardless of coastal visits. In other words, visit frequency is positively associated with better health, irrespective of income. Although the same number of visits does not reduce health inequalities, increasing the frequency of coastal visits may still provide “leverage points for intervention”12 to improve health for people of all of incomes; and when targeting groups with lower incomes, such interventions can ultimately reduce income-related health inequalities.
Although this study contributes to understanding the value of coastal contact for health, we recognize several limitations. First, as the data are cross-sectional, we cannot rule out that healthier individuals are more likely to live near the coast and visit it more often. Nevertheless, the data are consistent with longitudinal and intervention studies that suggest that exposure to the coast is causally associated with improvements ranging from momentary moods to longer-term health effects26. Hence, the current results cannot be dismissed on selective migration grounds alone.
Second, the data are limited to middle- and high-income countries. Future research should aim to investigate whether the coastal contact-health relationships also hold for low-income countries. As individuals in low-income countries disproportionally experience threats to their health from marine environments (e.g., due to marine pollution, poor water quality, parasites, and risk of drowning27), the coast may be seen as a health risk rather than a health-protective factor.
Third, the surveys were internet-based, which appear to have, for example, under-sampled individuals with low incomes28. The findings regarding the equigenesis hypothesis should, therefore, be treated with caution, and future research should attempt to collect samples that are representative of the population in terms of household income. Relatedly, the samples were representative in terms of age, sex, and region at the national but not sub-national level. Future studies may, therefore, aim to collect larger samples that are representative at the sub-national level and assess respondents’ ethnic background, to better understand whether the current findings hold for individuals living in different regions and environments (e.g., urban vs. rural areas) as well as for individuals with different ethnic backgrounds.
Forth, the surveys were limited to rather general self-reported measures. For policy recommendations, it would be important to test the current findings’ robustness using objective health measures (e.g., hospitalizations, health service utilization). Future studies may also include (self-reported) travel time to the coast as an additional indicator of perceived coastal accessibility that may be an ecologically more valid indicator than distance per se. In addition, the self-reported visits measure may be subject to memory biases; for example, reported visit frequency in the past 12 months may be higher at the beginning of fall when thinking back to summer compared to spring when thinking back to winter. Although the number of reported visits (in the past four weeks) remains relatively frequent even in fall and winter29, future studies may aim to collect data several times a year to smooth out potential seasonality biases.
Lastly, the surveys did not monitor coastal quality. Previous research shows that higher objective and perceived quality of green spaces are associated with better self-reported general health30. As this may also apply to coastal environments, we recommend that future research considers measures of coastal quality at national and regional levels.