In light of growing evidence for the antidepressant efficacy of psilocybin therapy26, the present findings advance our understanding of its possible underlying brain mechanisms. Across two trials, decreased brain modularity was observed and correlated with improvements in depressive symptomatology. Moreover, this antidepressant action may be specific to psilocybin therapy, as no changes in modularity were observed with the conventional SSRI antidepressant, escitalopram.
Research into the acute brain action of psychedelics has revealed well-replicated changes in global brain function that are somewhat consistent with those observed here (an increased repertoire of inter-regional and between-network functional connectivity (FC)29,30,31). A previous analysis of ours had suggested some contrasting changes in the architecture of spontaneous brain function 1 d following psilocybin treatment for depression relative to what has been observed during the acute psychedelic state itself: spatially expanded DMN FC (1 d after treatment for TRD) versus acute DMN ‘disintegration’25. However, others have reported evidence of increased inter-network FC 1 week and 1 month after psilocybin treatment35, as well as 1 d after ayahuasca, including increases in DMN-SN FC in healthy volunteers36. These findings are consistent with the present study, but here we show robust and reliable evidence that increases to global brain network integration accompanies the antidepressant efficacy of psilocybin therapy.
The present modularity metrics may be more sensitive indices of the antidepressant action of psilocybin than previously applied time-averaged within-network and between-network FC analyses25. Indeed, they may bear relevance to other FC metrics applied to acute-state psychedelic fMRI data29,30 where a general picture of increased global FC and a broadened dynamic state space has emerged28. In this context, the results could be understood as a ‘carryover’ effect resembling brain dynamics associated with the acute action of psychedelics, albeit at an attenuated level and in a specific population (depressed patients). To show robustness to analytical method, we also carried out more traditional mass-univariate analyses and these yielded consistent findings (Supplementary Figs. 3 and 4). However, an advantage of network modularity is its capacity to elegantly summarize global changes in the brain’s functional network organization37.
Previous research on resting-state activity in depression has found heightened network modularity correlating with symptom severity17,38. Additional work implies heightened within-DMN FC and elevated FC between limbic regions such as the amygdala, and high-level cortical regions correlates with ruminative symptoms in depression12,39. Taken together, a model emerges of abnormally modular spontaneous brain function in depression that is effectively remediated by psilocybin therapy. According to various findings, the FC energy landscape or state space in depression can be described as abnormally constricted, paralleling the narrow, internally focused, ruminative quality of mood and cognition in the disorder11. In contrast, psilocybin seems to increase the brain’s ability to visit a broader state space, both acutely and after psilocybin therapy in patients who are depressed, as shown here. Moreover, this ‘liberating’ action of psilocybin is paralleled by subjective reports of ‘emotional release’40,41 as well as subacute increases in behavioral optimism9, cognitive flexibility42 and psychological flexibility after taking a psychedelic drug43. Indeed, heightened emotional responsiveness may be specific to psilocybin therapy versus SSRIs26.
It is plausible that this putative liberating effect of psilocybin on cortical activity occurs via its direct agonist action on cortical 5-HT2A receptors, dysregulating activity in regions rich in their expression. We surmise that chronic escitalopram does not have the same effect on brain modularity due to its more generalized action on the serotonin system and predominant action on inhibitory postsynaptic 5-HT1A receptors, which are richly expressed in limbic circuitry27,44.
Beyond the global decrease in network modularity after psilocybin, we observed functional changes in DMN, EN and SN dynamics that are consistent with neurobiological models of depression45. These high-order transmodal networks house the highest density of 5-HT2A receptors, the principal action site for serotonergic psychedelics22,23. Higher-order networks are implicated in the acute action of psychedelics, where they show reduced modularity and increased communication with regions ordinarily outside of their community limits29,30,31.
The EN and SN have been associated with tasks requiring cognitive flexibility such as learning and task switching18,19,46,47; impaired functioning of these networks have been reported in depression14,17 and other disorders exhibiting cognitive inflexibility such as autism spectrum disorder48 and obsessive–compulsive disorder49. Our results suggest that decreased modularity or increased flexibility of these networks following psilocybin therapy is a key component of its therapeutic mechanism of action. We did not formally assess cognitive flexibility in the clinical trials reported here but we did observe improvements in general cognitive functioning after psilocybin treatment in the DB-RCT, as well as treatment-specific improvements in ‘emotional avoidance’ (an inversion of the related construct ‘psychological flexibility’26).
It should be noted that psychological processes that do not reliably relate to brain modularity changes may have played a role in the main clinical outcomes of this study, and an inability to discount such factors precludes the making of confident inferences that drug alone was the main causal determinant of the imaging outcomes or, indeed, that decreased modularity is sufficient for response to psilocybin therapy. Nevertheless, the changes observed in the neuroimaging data were consistent with previous brain imaging research regarding the acute action of psychedelics and are plausible in light of evidence of elevated modularity and abnormal functioning of higher-order networks in depression12,17,38,39,50.
Successful phase III DB-RCTs will be required to achieve licensing for psilocybin therapy, but pragmatic trials may better address questions regarding treatment practicability, specificity and optimization51. Given the emerging research into psychedelic therapy, it is important for large-scale trials to establish the generalizability, reliability and specificity of psilocybin’s antidepressant response. For example, it is likely that efficacy will depend on symptom severity, depression subtypes and comorbidities, as well as other key pharmacological and extrapharmacological factors52. For brain imaging studies, we would recommend network modularity analyses such as those employed here. fMRI datasets are complex, burdensome and susceptible to noise, contributing to the challenge of detecting reliable biomarkers. Simplifying composite measures, such as network modularity, combined with a research domain, symptoms-based approach to psychological phenomena, may be a particularly productive way forward37,51.
It should be noted that the present study’s findings do not support baseline modularity as a predictor of response to psilocybin therapy. Patients with a range of baseline modularity values showed modularity reductions after treatment with psilocybin; however, the present results do suggest that the early-phase modularity change is predictive of the long-term treatment response to psilocybin therapy.
It is noteworthy to consider the potentially confounding effects of head motion when interpreting fMRI data. Here, a robust fMRI preprocessing pipeline was employed alongside strict head motion criteria for patient inclusion. To examine robustness to motion, an analysis of head motion was conducted and is available in the Supplementary Information. These analyses bolster the present findings, as there was no evidence that head motion differed between sessions or treatment arms or that it correlated with network modularity. The fMRI data were collected with an eyes-closed protocol, which has some advantages; however, it would be compelling if these findings were replicated in data acquired with an eyes-open protocol. In-scanner sleep can be more likely during eyes-closed fMRI, which is a particular disadvantage53. In-scanner sleep cannot be ruled out here. However, the head motion analyses make it unlikely that sleep was a confounding factor. Furthermore, a self-reported visual analog scale of time spent asleep and ‘sleepiness’ were acquired immediately after all scan runs in study 2. An analysis of these data is available in the Supplementary Information. Critically, ratings of in-scanner sleep or sleepiness were low and did not differ between treatment arms or scanning session.
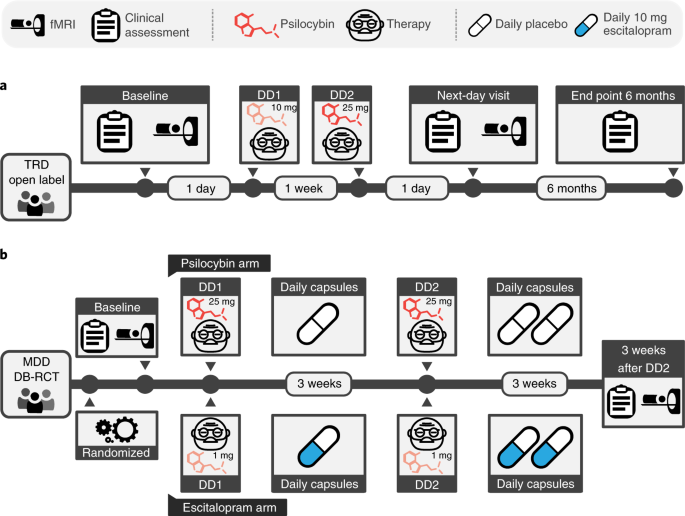
This study’s primary hypothesis was confirmed and replicated despite substantial differences between the design of the two trials. Baseline depression severity was significantly greater in the open-label trial. Furthermore, the open-label trial post-treatment fMRI scan was only 1 d after DD2 and was recorded with a 12-channel head coil and a 2-s repetition time (TR). In contrast, the DB-RCT post-treatment scan was conducted 3 weeks after DD2 and was recorded with a 32-channel head coil and a 1.25-s TR.
Acknowledging these differences between the trial designs serves to strengthen the validity of the main findings, as they were robustly replicated; however, the lack of replication in the finer-grained cartography analyses limits the network-specific inferences. A supplementary analysis (Supplementary Information) did confirm that baseline depression severity correlated with within-DMN connectivity and between-network DMN-EN and DMN-SN connectivity, as has been previously reported12,17,38,39,50; however, in the DB-RCT, we did not replicate the entirety of the changes in network cartography that were observed in the open-label trial. Given that the observed network effects directly follow predictions from the depression literature, it may be that they are more pronounced in more severe cases, such as those included in the open-label TRD trial. Alternatively, it may be that these effects are only detectable in a short-term, subacute phase after psilocybin therapy and not, for example, 3 weeks later. Parsing the relative contribution of baseline severity and time since treatment will be an important feature of future clinical trials with neuroimaging, ideally with larger samples and repeated scanning sessions.
Dynamic analyses can be challenging to conduct. To be sufficiently powered, time series need to be of sufficient length to be split into multiple time windows that are themselves sufficiently long to compute reliable FC measures, and previous research guided our selection of parameters54,55. Collecting sufficient fMRI data in patient cohorts can be challenging, but given the appeal of dynamic analyses, efforts are underway to facilitate and improve them54. It should be noted that a sufficiently broad window of time was used to estimate Pearson correlation FC; however, ongoing work is required to better understand how to capture the most functionally meaningful dynamic data.
With these caveats entered, it should be emphasized that the inferences from both cartography analyses converged on the brain’s higher-order networks. In particular, the DB-RCT analyses showed robust correlations (r~0.8) between increased higher-order network flexibility and psilocybin’s treatment response, and this converges with the open-label trial as well as previous research14.
In summary, depression is a major public health problem associated with huge burden and cost. Here, we identify a robust, reliable and potentially specific biomarker of response to psilocybin therapy for depression. Our results may help to explain why psilocybin therapy holds promise as a new treatment option in psychiatry.