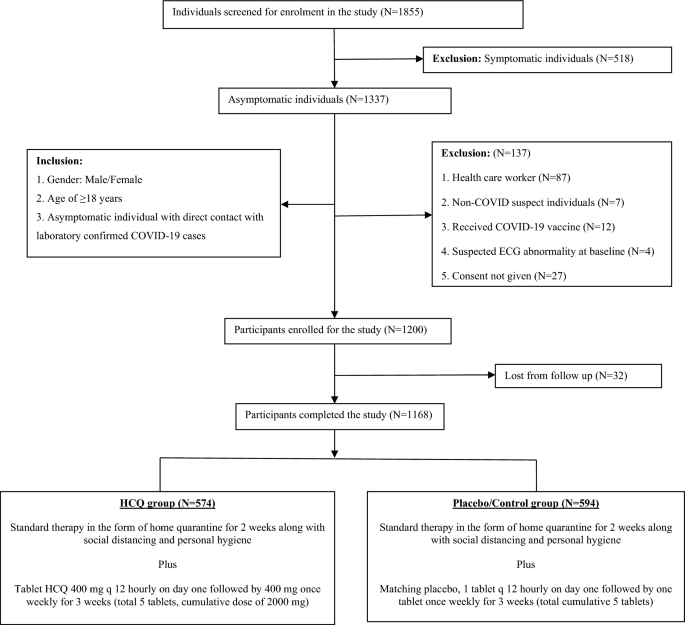
In this randomized, double-blind placebo-controlled clinical trial, 1168 asymptomatic individuals of high risk household direct contact with the laboratory-proven COVID-19 cases received PEP with either HCQ or Placebo and followed up for 4 weeks for the detection of new onset COVID-19. We found that PEP with HCQ was not associated with significant reduction in incidence of new onset COVID-19 as compared to the Placebo. Vaccines against COVID-19 came with great hope for the prevention of COVID-19 as well as reduction of the severity of illness and subsequent decrease in mortality. Even after more than a year of vaccine roll-out, many countries are going through multiple waves of the pandemic adding further assault to already traumatised human lives. Despite covering more than 66% of the population with full 2-dose vaccination, countries like the USA, UK and India have no respite from the surge of new COVID-19 cases1. On the other hand, India, despite administering more than 2048 million doses of vaccine, could be able to cover only about 67% of its population with full vaccination, as of 1st August 20221. It was because of huge number of population, and still around 20 thousands new cases being reported daily in India1. As of 28th July 2022, the USA was able to cover more than 32% of the population with booster doses of vaccination, but still reporting more than 100 thousand new cases daily1.This was more because of rising numbers of mutated variants of the SARS-CoV-2, rendering neutralizing antibody less effective against it, and decreasing effective vaccine efficacy at the ground level26,27. As the majority of COVID-19 patients are asymptomatic, hardly requiring hospitalization, prevention of COVID-19 in high-risk individuals is the upmost priority to restrain this devastating pandemic. An anti-viral drug effective against SARS-CoV-2 is the need of the hour along with mass vaccination to combat this pandemic more efficiently to put an end to the ongoing human misery. Mass production as well as distribution of drugs to the poorest sections of society is much easier than complex vaccine manufacturing leading to better coverage against COVID-19. Oral antiviral drugs, Paxlovid, Molnupiravir received emergency use authorization from the US FDA for mild to moderate COVID-19, as it was found to reduce the risk of hospitalization or mortality8,9. But for the prevention of COVID-19, PEP with Paxlovid was found to be ineffective and the role of PEP with Molnupiravir is still inconclusive8.
HCQ generated sense of belief for the treatment and prevention of COVID-19 due to its in vitro virucidal action against SARS-CoV-228. Hydroxychloroquine (HCQ), a less toxic derivative of chloroquine (CQ) is part of the 4-aminoquinoline family compounds29. HCQ was initially used as an anti-malarial agent and presently is best recognized as an immunomodulatory and anti-inflammatory agent for the treatment of autoimmune diseases likes rheumatoid arthritis and systemic lupus erythematosus. The proposed primary mechanism for anti-viral action of HCQ is alkalinization of endosomes and lysosomes and subsequent rise in pH leading to inhibition of viral nucleic acid replication, protein glycosylation, viral assembly and transportation, and release of new viral particles28,29. Additionally, HCQ can also block viral uptake by inhibiting the glycosylation of the ACE-2 receptor at the plasma membrane to which viral spike protein binds for cellular entry29. Further, the immunomodulatory action can also limit the hyperimmune and inflammatory response of COVID-1930,31. The Omicron has improved ability to enter cells via endosome and HCQ has the potential against Omicron variant of SARS-CoV-2 through alkalinization of endosomes, preventing membrane fusion. But this hypothesis is yet to be proven by clinical trials.
Presently evidence emerged against the therapeutic benefit of HCQ in hospitalised COVID-19 patients in term of recovery and prevention of mortality21,22. But the role of HCQ as PEP for the prevention of COVID-19 remained uncertain when the study was conducted. ICMR data from multiple national institutions, as well as our institutional data were supportive for PEP with HCQ for the prevention of COVID-1917,18. There was also lack of RCT, done on Indian population regarding PEP with HCQ. Majority of the studies which produced evidence in favour of HCQ for the prevention and treatment of COVID-19 were either observational or retrospective in nature13,18,24,25. So far, Boulware et al. was the largest RCT which concluded that PEP with HCQ was not beneficial for the prevention of COVID-1921. However, concerns were raised regarding study design, methodology, and case definition. In this study, the time interval for intervention (exposure & recruitment to 1st dose) was significantly prolonged (> 72 h) in majority of the participants. Delayed intervention may render the drug less efficacious for the prevention of COVID-19 and rather turnout to be more about treatment or prevention of progression of COVID-1925. The study population of the present RCT was larger and all the participants received their 1st dose of HCQ within 24 h of proven exposure during their hospital visit with family members or friends for any medical emergency or COVID-19 related work-up. This enabled us, majority of participants to receive their 1st dose under direct observation therapy (DOT) at the time of enrollment itself.
Boulware et al. defined COVID-19 cases as symptomatic illness supported by a positive molecular assay or COVID-19-related symptoms, but asymptomatic presentation of COVID-19 is also very frequent3. This was a probable reason for detecting very few number PCR-confirmed COVID-19 cases (16 of 107 symptomatic cases), missing asymptomatic cases. In the present study RTCPR for SARS-CoV-2 RNA was performed in both symptomatic and asymptomatic individuals and was able to detect asymptomatic COVID-19 cases also. According to our study, 20% (10 out of 51) of COVID-19 cases were asymptomatic.
In Boulware et al. the majority (66.4%) of participants were HCW. There is still scarcity of RCT, exploring PEP with HCQ for the prevention of SARS-CoV-2 infection in high-risk household direct contacts of COVID-19 cases. The present study aimed to evaluate the efficacy of HCQ as PEP for prevention of COVID-19, particularly in asymptomatic household direct contacts of the laboratory-confirmed COVID-19 cases. Though, the HCW related to COVID-19 patient care and the household direct contacts of COVID-19 cases are at risk for SARS-CoV-2 infection, they have a comparatively different risk category. HCWs are expected to participate in COVID-19 patient care after wearing personal protective equipments, usually for a fixed duty hours, and can retain a safe distance from the patients as per feasibility. The household contacts get exposure to COVID-19 unknowingly without any precautions or personal protective equipment, as the patients are either family members or friends or relatives, and they live with COVID-19 patients for days to weeks without retaining a safe distance. Therefore, household direct contact possesses a greater risk for COVID-19 compared to HCW and incidence of COVID-19 after exposure may differ in HCW and household direct contact. So the HCW were excluded from the present study.
In a household RCT, Barnabas et al. concluded that PEP with HCQ was not efficacious for the prevention of COVID-1932. However, the sample size was smaller; the study did not exclude HCW and more significantly, the time interval from enrollment to the intervention was more than 48 h due to the remote recruitment of participants. The cumulative dose of HCQ was also higher (3400 mg) leading to a higher incidence of ADR.
Additionally, a Cluster-Randomized Trial concluded that PEP with HCQ did not prevent SARS-CoV-2 infection in asymptomatic direct contact of COVID-19 cases33. However, it was not a blinded study and majority of the participants received delayed HCQ intervention > 72 h of proven contact. Further published RCT also emphasized that HCQ prophylaxis was not beneficial for the prevention of COVID-19 but again it was done on HCW with very little sample size due to early termination of the study34. Another RCT found ineffectiveness of HCQ for prevention of COVID-19 in HCW who received HCQ of 400 mg weekly or twice-weekly35. But, this study also raised questions regarding the dose of HCQ for prophylaxis as it achieved very low therapeutic blood concentrations leading to its failure35.
Safety has always been a concern against the use of HCQ as it can cause life-threatening cardiac arrhythmias, QT prolongation, retinopathy causing loss of vision, hypoglycaemia, and haemolysis in G6PD-deficient patients. However, these side effects are not common in conventional practice and HCQ has been found to be safe with prolonged lifelong use in rheumatoid arthritis and systemic lupus erythematosus36,37. In the present study, none of the participants had serious ADR. The drug was tolerated well in most of the participants with good compliance and was found to be safe. Most commonly reported ADR was mild gastritis-related symptoms on day one or two after receiving 800 mg of loading dose, which responded well with antacid without any recurrence thereafter. Though one participant reported an episode of palpitation, it resolved spontaneously, lasting for less than a minute without any recurrence. The incidence of ADR was higher in the studies by Boulware et al. and Rajasingham et al., probably due to higher cumulative dose (3800 mg and 5600 mg to 10,400 mg respectively) of HCQ compared to the present study (2000 mg)21,35.
HCQ was also tried unsuccessfully against the previous corona virus pandemic (MARS) and perhaps COVID-19 is not the last corona virus pandemic either. Despite the unfavorable results of HCQ for the treatment and prevention of COVID-19, the practice of irrational use of HCQ for the prevention of COVID-19 still continues in many countries31. The advisory and indiscriminate use of HCQ for COVID-19 had been predominantly under the influence of fear for SARS-CoV-2 infection and social media forces rather than evidence based on clinical research outcomes. Perhaps, this study probably put an end to the era of controversy with HCQ for the prevention of COVID-19. With multiple clinical trials showing evidence against HCQ, the ICMR withdrew HCQ for the management or prevention of COVID-19 in August 202138.
HCQ remains a myth only as it couldn’t produce sufficient in vivo evidence in favor of its benefit against COVID-19. But, at the same time it opens the gate for further research in search of newer and efficacious anti-viral drugs or repurposing of the established drugs against SARS-CoV-2 making us more efficient in defeating this ongoing pandemic. Till then, vaccination, increasing social awareness about the disease and better adherence to the use of face mask, maintaining adequate social distancing and hand hygiene are the best way for the prevention of COVID-19, breaking the chain of transmission of COVID-19 in community39.
Limitation of the study was, being a single center clinical trial raised doubt regarding the representation of large diverse Indian population. However, being a tertiary care center, the PGIMER caters to multiple states which include Punjab, Haryana, Himachal Pradesh, Uttarakhand, Uttar Pradesh, Jammu & Kashmir, Rajasthan and Bihar, representing large and diverse parts of India.
The event number (primary end point) was lower than expected. The sample size may have been inadequate to exclude small but clinically meaningful decreases in the incidence of SARS-CoV-2 infection in high risk individuals.
Follow-up ECG could not be done to detect new onset QT prolongation. Only one patient had a self-limiting episode of palpitation without recurrence, and none of the participants reported any symptoms related to any acute cardiac events.
Majority of the participants represented a younger (18–45 years) age group (84.4%) with less representation for older age groups who may have contrasting risk factors for COVID-19 than younger population, and only 3 participants from > 45 years age group had COVID-19 (Table 3). But the incidence of COVID-19 was comparable in different age groups in the present study (Table 3).
In conclusion, PEP with HCQ is not advantageous for the prevention of COVID-19 in asymptomatic household direct contact of the laboratory-confirmed COVID-19 cases. Though HCQ is a safer drug, the practice of irrational and indiscriminate use of HCQ for COVID-19 should be restrained with better pharmacovigilance till further supportive evidence emerges. Till then, mass vaccination, increasing social awareness and use of face masks, social distancing and personal hygiene are the best ways for the prevention of COVID-19.