The main lessons learned from this work are that, contrary to expectations, many post-COVID-19 patients directly contacted the coordination team without going through their attending doctor. Further, the majority had significant pre-existing comorbidities; their main symptoms were those previously described, with fatigue being largely predominant. Despite the willingness to help patients and their participation in the therapeutic action proposed, with the noticeable exception of dyspnea and chest pain, which decreased significantly, self-reported patients’ symptoms often persisted and approximately one third of them were not back at work almost two years after the initial infection.
Interestingly, the population did not totally fit with the expected characteristics of non-hospitalized patients. Although there was a majority of relatively young persons with an average age of 49 years, including a high proportion of women for whom sex was proposed to be a risk factor for several long-term post-COVID symptoms [ 12 ] and who experienced no hospitalization due to SARS-CoV-2, many of the patients were not healthy before SARS-CoV-2 infection. Additionally, the delay since COVID infection was around 15 months, suggesting that such complex situations did not resume earlier, as generally occurs. The symptoms presented by the patients had no specificity except for their very long duration [ 2 15 ].
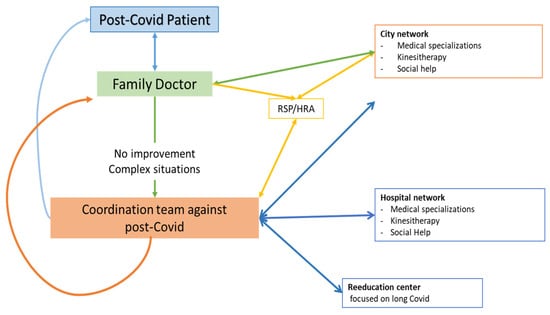
Alternatively, although meetings with city practitioners does not seem to favor this hypothesis, this might not reflect the entire population suffering from intense post-COVID-19 condition, and one might think that all patients had no access to the coordination team. Supporting such an idea, contrary to the initial intention, treating physicians addressed the patients to the coordination team only in 27% of the cases. Thus, most patients went directly to the coordination team or through other medico-social structures. While this interpretation needs to be approached with caution, patients’ need for further medical or social support might have been more important than previously thought by their physicians.
During this seven-month period, 105 patients contacted us directly or through their treating physicians or a medico-social structure. This number appears relatively small, but for posterity, only complex situations should have been referred, i.e., patients for whom the attending physicians could not find adequate solutions within a reasonable time. It suggests that many patients have benefitted well from the support given by their treating physician, the cornerstone of the system in France. Accordingly, the 51 patients who had not completed their file had likely obtained adapted answers to their questions upstream, without needing to fully benefit from the network set up by the coordination team.
4.2. Therapeutic Proposals and Perceived Efficacy of the Support
17, In all cases, with the consent of the patients, we included their referring physicians in the process, to afford that they remained the cornerstone in patient management. The precise knowledge of the attending physician of the social context of the entire family and the patient’s environment allows a better approach of everyone’s singularity. In view of the main symptoms observed and of the investigations and therapies already performed, after excluding severe diseases needing emergency support, the coordination team mainly proposed focused rehabilitation protocols. In view of the adapted rehabilitation programs, performed in specialized teams, we rather expected improvements in patients’ symptoms. Indeed, early rehabilitation is the key therapy for COVID patients [ 16 18 ]. Organ-related symptoms such as chest pain and dyspnea significantly decreased after re-education, suggesting therapeutic efficacy.
However, as observed during the second phone call, not all patients reported improvement, either total recovery (4%) or moderate improvement (33%). Thus, more than half of patients showed no or very little improvement (20% and 38%, respectively).
A possible explanation might be diseases pre-existing before SARS-CoV-2 infection. Thus, management of these conditions could not be optimal, resulting in patients’ symptom persistence. Indeed, many patients had relatively important comorbidities prior to SARS-CoV-2, affecting the cardiovascular, respiratory, systemic and musculoskeletal systems. Further, several patients had a history of cancer or psychiatric disorder. When talking about post-COVID-19 condition, there is a lack of data reporting reduced functions and activity in the participants compared to the previous ones, i.e., before SARS-CoV-2 infection, and further studies will be useful to investigate such issues.
We nevertheless investigated whether symptom persistence was related to pre-existing pathologies. Indeed, SARS-CoV-2 infection might modulate, or generally enhance symptoms, but as previous diseases persist, symptoms should also persist even if specific recovery from SARS-CoV-2 occurs. No clear relationship between pre-existing diseases and SARS-CoV-2-associated symptoms was observed, which is consistent with an interesting recent report supporting that comorbidities before SARS-CoV-2 did not predict persistent symptoms [ 19 ]. Further, fatigue, which was one of the more frequent symptoms, has been shown to be not related to SARS-CoV-2 severity [ 20 ]. On the other hand, we observed a tendency to a greater return to work if patients were healthy before SARS-CoV-2 infection. Unfortunately, these are few and the hypothesis that return to work is easier in patients who do not have comorbidity remains to be demonstrated.
22,23, Alternatively, many studies are on the way to better understanding SARS-CoV-2 pathophysiology, including the potential involvement of immune, cardiac, vascular, etc., alterations [ 21 24 ] that might participate in long and complex SARS-CoV-2 symptoms and generate adequate treatment.
Finally, the authors also proposed that psychological factors might play a role in post-COVID-19 condition since the remaining symptoms (fatigue, neurocognitive disorders, pain) were very general and impacted by the patients’ subjective feelings—potentially and partially disconnected from the degree of the disease. This is largely controversial and generally badly received by the patients, who claim that they are not believed. In this view, the large reduction in anxiety we observed also suggests beneficial effects secondary to psychologic support. Thus, psychological and physical supports should not be in opposition, as both ways deserve to be used to better fight against post-COVID-19 condition. We wish to emphasize that although difficult to deal with, their feelings are a reality for the patients, and it is important for medical teams to consider them and try to improve such feelings.