UK Biobank population
The UK Biobank is a prospective cohort for the investigation, prevention, diagnosis and treatment of chronic diseases, such as CV diseases in adults. 502,478 Britons across 22 UK cities from the UK National Health Service Register were included between 2006 and 2010. The cohort was phenotyped and genotyped, by participants who responded to a questionnaire; a computer-assisted interview; physical and functional measures; and blood, urine, and saliva samples23. Data included socio-economic, behavior and lifestyle, mental health battery, clinical diagnoses and therapies, genetics, imaging and physiological biomarkers from blood and urine samples. The cohort protocol can be found in literature24.
Ethical considerations
All participants provided electronic informed consent and UK Biobank received ethical approval from the North-West Multi-center Research Ethics Committee (MREC) covering the whole of UK. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the North West—Haydock Research Ethics Committee (protocol code: 21/NW/0157, date of approval: 21 June 2021). For details: https://www.ukbiobank.ac.uk/learn-more-about-uk-biobank/about-us/ethics.
Study population
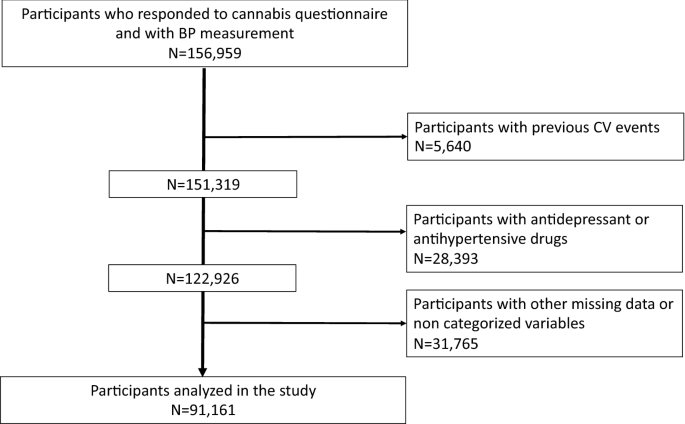
156,959 volunteers of the UK Biobank who responded to the question of cannabis use and with BP measurement were recruited. Of them, we excluded 65,798 for data missing and not categorized variables and excluding participants with antihypertensive drugs, antidepressant drugs and previous CV events (Supplementary Table 1). CV events were excluded from the analyses due to the inconsistent role of cannabis in CV disorders25. Antidepressant drugs use were excluded due to the association between cannabis use and depression26. The list of antidepressant drugs was available at27. We therefore analyzed 91,161 volunteers (Fig. 1).
Blood pressure measurement
Systolic and diastolic blood pressure (SBD, DBP) were measured twice at the assessment center by the use of an automated BP device (Omron 705 IT electronic blood pressure monitor; OMRON Healthcare Europe B.V. Kruisweg 577 2132 NA Hoofddorp), or manually by the use of a sphygmomanometer with an inflatable cuff in association with a stethoscope if the blood pressure device failed to measure the BP or if the largest inflatable cuff of the device did not fit around the individual’s arm28.
The participant was sitting in a chair for performing all the measures. The measures were carried out by nurses trained in performing BP measures29. Multiple available measures for one participant were averaged. The Omron 705 IT BP monitor has satisfied the Association for the Advancement of Medical Instrumentation SP10 standard and was validated by the British Hypertension Society protocol, with an overall “A” grade for both SBP and DBP30. 5295 participants (5.8% of the study population) had a manual sphygmomanometer BP measurement. Nevertheless, automated devices measure lower BP in comparison to manual sphygmomanometers31, thus, and according to previous works for UK Biobank data32,33,34, we adjusted both SBP and DBP which were measured using the automated device using algorithms:
For SBP, we performed the following algorithm:
$$SBP=3.3171+0.92019\times SBP \left(mmHg\right)+6.02468\times sex \; (male=1; \, female=0)$$
For DBP, we performed the following algorithm:
$$DBP=14.5647+0.80929\times DBP \left(mmHg\right)+2.01089\times sex \; (male=1; \, female=0)$$
Pulse pressure (PP) was calculated as = SBP − DBP.
Cannabis use
Cannabis use was reported by self-reported questionnaire. Participants were asked about their cumulative lifetime cannabis use: ‘Have you taken cannabis (marijuana, grass, hash, ganja, blow, draw, skunk, weed, spliff, dope), even if it was a long time ago?’. Those who responded ‘no’ were classified as controls and those endorsing ‘yes’ options were classified as cannabis users. We separated these users into three groups according to categories reported in the questionnaire: those reporting initial cannabis use (‘yes, 1–2 times’, ‘yes, 3–10 times’) and continued cannabis use (‘yes, 11–100 times’: moderate users; ‘yes, more than 100 times’: heavy users). Cannabis users were asked “About how old were you when you last had cannabis?”. Cannabis user participants reporting this information and showing difference between age at inclusion and age of last cannabis use strictly inferior to 1 year were classified as “current users”, the others as “past users”. Among cannabis users, participants were asked about their cannabis frequencies use during taking: ‘Considering when you were taking cannabis most regularly, how often did you take it?’. The participants were classified into four groups, as: ‘every day’, ‘once a week or more, but not every day’, ‘once a month or more, but nor every week’, ‘less than once a month’.
Covariates
Diabetes status was defined on either receiving anti-diabetic medication or diabetes diagnosed by a doctor or a fasting glucose concentration ≥ 7 mmol/L. Dyslipidemia was defined as having a fasting plasma total-cholesterol or triglycerides level of ≥ 6.61 mmol/L (255 mg/dL) or > 1.7 mmol/L (150 mg/dL) respectively or having statins medication35. Hypertension was defined as systolic blood pressure (SBP) at least 140 mm Hg and/or diastolic BP (DBP) at least 90 mm Hg36. Medications were characterized by the question: “Do you regularly take any of the following medications?”.
Current tobacco smokers were defined as participants who responded “yes, on most or all days” at the question “do you smoke tobacco now”. CV diseases were defined by heart attack, angina and stroke, as diagnosed by a doctor and reported in questionnaires. Body mass index was calculated as weight (in kg) divided by height2 (meter), and categorized as high (BMI > 30 kg/m2), moderate (BMI between 25 and 30 kg/m2) and low (less than 25 kg/m2). Biological parameters were detailed in the UK Biobank protocol37. Education level was defined in three categories high (college or university degree), intermediate (A/AS levels or equivalent, O levels/GCSEs or equivalent), and low (none of the aforementioned)38. Income level was defined as, high level (‘greater than £52,000 per year’), moderate level (between £18,000 and £51,999 per year), and low level (‘less than £18,000 per year)39. Alcohol level consumption was defined as reported in questionnaire: high level (‘daily or almost daily’), moderate level (‘three or four times a week’, or ‘once or twice a week’, or ‘one to three times a month’), and low level (‘special occasions only’ or ‘never’).
Statistical analysis
Characteristics of the study population were described as the means with standard deviation (SD) for continuous variables. Categorical variables were described as numbers and proportions. Comparisons between groups were performed using Student’s test for continuous variables. Pearson’s χ2 test was performed for categorical variables. Statistical analyses were stratified on gender since blood pressure differs between men and women40 and a difference in cannabis consumption between gender41.
Firstly, this study explored the association between cumulative lifetime cannabis use and BP levels, secondly, the current or past use of cannabis consumption with BP and then, the frequency of cannabis use during taking with BP.
Associations between cannabis use and BP levels were examined with linear regression models computing regression coefficients (b) and their standard errors (SE). Firstly, gender models were adjusted for age. Secondly, gender models were adjusted for age, education, income level, alcohol consumption, tobacco habits, BMI categories, diabetes and dyslipidemia. “Never users” was considered as the referent group in the analyses. Subgroup analyses by education, income level, BMI, diabetes, dyslipidemia, alcohol and tobacco habits were performed. Interactions were examined by including simultaneously cannabis use status and one of the covariates, their interaction term and adjustment for all other covariates. Statistics were performed using SAS software (version 9.4; SAS Institute, Carry, NC). A p value < 0.05 was considered statistically significant.
Informed consent
Written informed consent has been obtained from the patients.