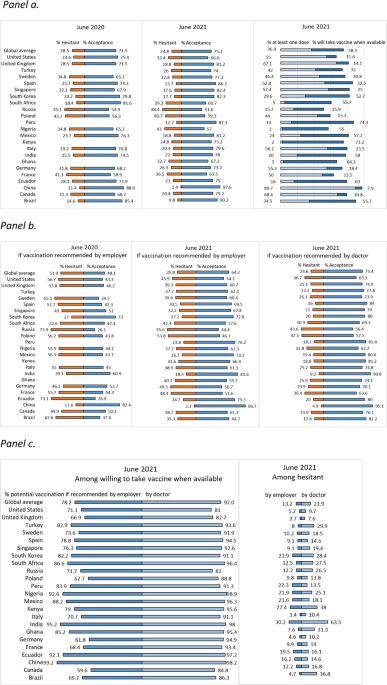
Reported COVID-19 vaccine acceptance, measured by intention to get vaccinated or having received at least one dose of an available vaccine, increased over the last year in 15 of the 19 countries studied in 2020 and 20213, and was 75.2% for all 23 countries studied in 2021. However, this percentage is still below the estimates needed to control the pandemic29. Negative perceptions of safety, trust in the science behind vaccine development, and vaccine efficacy were the most consistent correlates of hesitancy. Government mistrust was associated with vaccine hesitancy in most countries. Other factors associated with vaccine hesitancy varied by country and included personal experience with COVID-19 (e.g., sickness or loss of a family member) and demographic characteristics (e.g., gender, education, and income).
In order to improve global vaccination rates, some countries may at present require people to present proof of vaccination to attend work, school, or indoor activities and events. Our results found strong support among participants for requirements targeting international travellers, while support was weakest among participants for requirements for schoolchildren. Support for requiring vaccines was substantially lower among those who were hesitant to get vaccinated themselves. Importantly, however, recommendations by a doctor, or to a lesser extent by an employer, may impact a respondent’s views on vaccination in some countries.
Misperceptions of vaccines as having high risks and low benefits is a driver of vaccine hesitancy30 that may also reflect a respondent’s lower trust in the science behind vaccine research and production21,31,32,33,34. In late 2019 and early 2020 the majority of people surveyed globally reported that science was important in their society. Perceived importance of science was described as valuing government investments in scientific research, believing it is very important to be a world leader in scientific achievement, and trusting scientists to do what is right for the public35. Our results corroborate these findings: negative perceptions of trust in science and vaccine safety and efficiacy were most strongly associated with vaccine hesitancy.
Health care workers are in a position of trust and are perceived as important sources of reliable and accurate vaccine information36,37,38,39. However, one study found that COVID-19 vaccine hesitancy among HCWs ranged widely between 4.3% and 72%, with an average of 22.5%40. The main reasons for vaccine hesitancy among HCWs are similar to those found in the general population: concerns about efficacy, safety, and potential side-effects. Demographic factors among HCWs such as male gender, greater age, and attainment of a doctoral degree were positively associated with acceptance of COVID-19 vaccines40. Our findings align with prior reports of higher rates of vaccine acceptance among physicians compared to nurses41,42,43,44. Among hesitant respondents in this survey, the advice of their physician improved willingness to accept a COVID-19 vaccine, as did recommendation by their employer, to a lesser extent.
In June 2020, one of the factors most strongly associated with acceptance of a yet unavailable vaccine was trust in government to successfully address unexpected health threats, such as the COVID-19 pandemic3. A 2020 study in Portugal, where 56% of respondents reported they would wait to take the COVID-19 vaccine and 9% of respondents reported they would refuse vaccination, showed that vaccine hesitancy was related to a poor perception of government and health service responses as well as a lack of trust in the information provided45, which is consistent with previous pandemic research46. Yet, after accounting for socio-demographic and COVID-19 experience variables, our study found mistrust in the central government was not significantly associated with vaccine hesitancy, as was also the case for the local government, in most countries sampled, except in Ghana and Poland. Respondents in Nigeria reported high vaccine hesitancy and high distrust in governmental ability to respond to COVID-1947, but the association between vaccine hesitancy and trust in government was not significant. This dissonance between trust in government and vaccine acceptance in our study could be related to the population’s general dissatisfaction with government responses to the pandemic and its economic consequences, with vaccine acceptance being independent of such sentiments and more a reflection of personal experiences with COVID-19 illness or loss of life and livelihood. Our results confirm that direct experience for self or family with the illness and/or loss of a family member to the disease are independently associated with vaccine acceptance.
As health systems in LMICs struggle to address COVID-1948, vaccine access has become a cause for national and international frustration. Most LMICs have been slow to receive and distribute vaccines, which are much more available in high-income countries, prompting critiques of global vaccine inequity49, which were exacerbated with the distribution of so-called booster shots in high-income countries in the autumn of 2021. Access issues, coupled with vaccine hesitancy, which this study found declined overall, can have catastrophic effects. In South Africa, where hesitancy increased compared to our 2020 study, data collection coincided with the rapid transmission of the Omicron variant. The virulence and transmissibility of future possible variants remain unknown, highlighting the need to augment efforts to increase vaccine equity and public trust in vaccination50.
Most recent studies do not investigate income as a potential influencer on vaccine acceptance. A study conducted in Portugal found that people who lost income during the pandemic were more hesitant45. A study carried out in Ireland showed that people with a lower income were also more vaccine hesitant51. A study carried out in China showed that loss of income was greater among residents of areas with more severe COVID-19 transmission and magnified existing social and economic disparities52. A study conducted in the US showed that having lower income was associated with a higher risk of depression during the pandemic53. Our results show that a lower household income is associated with a greater level of hesitancy in 11 countries, while a loss of income due to the pandemic is positively associated with vaccine acceptance in four countries. We suspect the perceived positive association between vaccination and desire for a “return to normalcy” is stronger among people who lost socioeconomic status and financial stability due to revenue loss.
Globally, anxiety and depression increased during the pandemic while positive emotions such as happiness and life satisfaction decreased54. A global review of COVID-19-related mental health studies found that the prevalence of anxiety ranged between 26.5%–44.6% and depression between 8.1%–25% and that the prevalence of insomnia was 38%55. Stress levels were found to vary widely (from 3.8% to 68.3%). In several countries such as Bangladesh, India, and Pakistan, cases of suicide linked to fear of COVID-19 have been reported54. Across a range of time points and geographies, people who had COVID-19 reported more symptoms of anxiety, depression, and post-traumatic stress disorder than people without a COVID-19 diagnosis54. Similarly, people with pre-existing psychiatric conditions reported a worsening of their psychiatric symptoms during the pandemic56.
Mental illness has been associated with a higher risk of COVID-19 related mortality and morbidity57, yet studies examining the impact of mental health on vaccine hesitancy are scarce. One German study did not show a relation between depression or anxiety and vaccine hesitancy58. This is in line with a Danish study showing that, although people previously diagnosed with mental illnesses reported slightly lower vaccine acceptance compared to the general population (84.8% versus 89.5%), vaccine hesitancy among people with mental illnesses did not seem to be a deterrant to reaching herd immunity59. In Ireland, by contrast, people who had received treatment for a mental health problem were more accepting of a vaccine, unlike UK respondents who showed no such association51. Our study results suggest that the effects of experience of depression and anxiety are far from universal, with divergent associations between anxiety and depression and vaccine hesitancy reported across the 23 countries. Future research should undertake a deeper examination of cultural influences on mental health-related vaccine hesitancy.
Increased vaccine scepticism may result from the dissemination of erroneous or inaccurate, and often politicized32,60, information. Misinformation is associated with vaccine hesitancy, undermining confidence in the safety and efficacy of COVID-19 vaccines61. For example, over two-thirds of vaccine related videos on YouTube that were analyzed for content accuracy in May 2019 presented unreliable safety and efficacy information62. However, in mid-February 2021, despite only 46% of Twitter poll respondents agreeing that all COVID-19 vaccines are safe, 83% indicated they would accept a vaccine, while only 2% would agree to accept one if mandated63. Our results indicate that vaccine hesitant respondents may be more willing to accept a COVID-19 vaccine if recommended by their doctor.
To control the COVID-19 pandemic, some countries have considered or implemented requirements for proof of vaccination, or vaccine mandates, to permit travel internationally or to attend work, school, or indoor events. Consistent with our results, other recent studies found higher support for vaccine requirements to travel internationally than domestically64,65. Also in line with our results, a September 2020 study from the US found that approximately half of the general population considered mandatory COVID-19 vaccination for children attending school acceptable, a category that also remains universally low in our sample (overall 58.2%)66.
Vaccine mandates for adults by state governments were considered acceptable by 40.9% of the US population, whereas 47.7% accepted mandates by their employer to attend work66. However, our 2020 global study showed that people were potentially more likely to accept voluntary over employer-mandated vaccination3. “Choice architecture” that frames vaccination requirements as effective public health and disease prevention and control tools, which one chooses to accept in order to fully participate in society, as opposed to a violation of the individual’s right to select medical treatment, may promote incremental vaccine uptake67. As vaccines receive full (i.e., no longer just emergency use) approval from regulatory agencies, this may lead to improved perceptions on safety and efficacy, and vaccination campaigns based on such choice framing could convince more unvaccinated adults and young adults to accept vaccination and increase parental acceptance of vaccination for their children.
One limitation of correlation analyses using actual vaccination rates is that countries with low vaccine access may produce unreliable results given this extrinsic factor. Additionally, our questionnaire asked about a general COVID-19 vaccine, whereas several COVID-19 vaccines, each with different efficacy results and targeted misinformation, are being distributed globally. This study is strengthened by maintaining a sampling methodology that ensured population representativeness between iterations. We tested COVID-VAC as a composite score, which showed high internal reliability and external construct validity with our measure for vaccine hesitancy among large nationally representative samples in 23 countries. Yet, other aspects of scale validation have not been conducted, such as test-retest reliability, responsiveness over time, and content validity to assess the potential exclusion of other relevant factors for vaccine hesitancy68, though authors consulted the SAGE Working Group framework of determinants and previous related studies to design the questionnaire. Items were written unambiguously and succinctly to adhere to questionnaire development best practices68, with the possible exception of item 5, “I trust that my government is able to deliver the COVID-19 vaccine to everyone, everywhere in my country, equally,” which may have introduced a response bias by referring to multiple actors and actions. We encourage further testing of this tool over time, in conjunction with emerging determinants of COVID-19 vaccine hesitancy69, and using modified items to reduce potential biases in order to fully understand its validity.
Although some countries are currently disengaging from aggressive COVID-19 control measures, the disease has by no means been subdued. For ongoing COVID-19 vaccination campaigns to succeed in improving coverage going forward, substantial challenges remain to be overcome. These include increasing vaccination among those reporting a lower vaccine confidence or who have difficulties in accessing vaccination services, in addition to expanding vaccine access to low- and middle-income countries. This study confirms the importance of a positive perception of vaccine safety and efficacy for vaccine acceptance under any circumstances. Ongoing vaccination requirements and active vaccine promotion are not without the risk of hardening opposition to COVID-19 vaccination, but the alternative is to risk future surges from new variants and the continuation of the pandemic as a public health threat. Further, misinformation continues to spread and can impact COVID-19 vaccine acceptance70. We still need accurate COVID-19 vaccine communication delivered by trusted sources to clearly explain vaccine safety and benefits to individuals, families, and society at large.