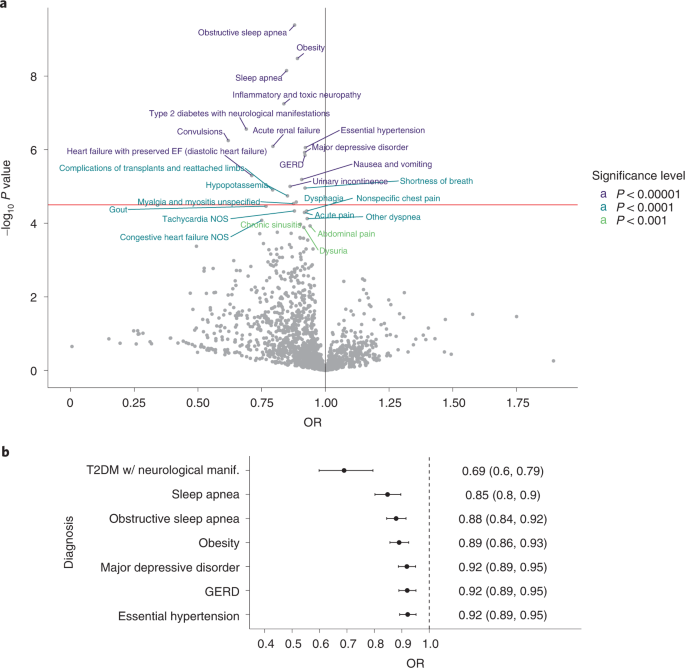
We examined the association between step count volume and intensity across the entire spectrum of human disease using commercial activity monitors linked to an individual’s EHR. We identified consistent and statistically significant associations between activity levels and incident diabetes, hypertension, GERD, MDD, obesity and sleep apnea. Taking more steps each day was related to lower risk of developing these chronic diseases. Higher step counts were associated with protection from obesity in a high-risk population (BMI 25–29 kg m–2). Step count was positively correlated with step intensity, regardless of the bout cadence definition. The relation of step counts with disease risk persisted for diabetes, GERD, MDD and sleep apnea even when adjusting for step intensity. Step intensity was also significantly associated with these outcomes. These data provide new, empiric evidence of activity levels associated with chronic disease risk and suggest that integration of commercial wearables data into the EHR may be valuable to support clinical care.
Our findings are consistent with previous literature describing associations between step counts and adverse events10,11. A systematic review by Hall et al.10 found that taking more steps per day was related to lower risk of all-cause mortality, cardiovascular events and incident diabetes. The National Health and Nutrition Examination Survey study, which quantified steps over a 7-day monitoring period and assessed mortality over an average of 10.1 years, found a 51% lower mortality at 8,000 steps per day compared with 4,000 steps per day1. Similar results were reported from a middle-aged, biracial cohort with 7 days of monitoring and over 10 years of follow-up time5. A prospective cohort study conducted in 3,055 community-dwelling adults aged over 70 years found a similar nonlinear relation between daily steps and risk of developing diabetes, where the risk leveled off at 8,000 steps per day12. It is notable that step count thresholds associated with risk of mortality and cardiometabolic disease in prior studies are similar to step count thresholds associated with a wide variety of previously unreported phenotypes in our study. These results suggest that a single step count target of approximately 8,000–9,000 steps per day may be suitable to reduce risk of many common conditions.
Our study design and analytic approach differed from prior studies in important ways that make our results new and clinically relevant. First, prior studies assessed step counts over a single, short (usually 7 days) monitoring period with activity data between the baseline monitoring period and outcomes assessment, often many years later. Short monitoring periods are prone to an observer effect and may not accurately reflect true short- and long-term activity behavior13. In contrast, our models accounted for changes in steps over the entirety of an individual’s monitoring period (median of 4 years) rather than a brief snapshot. Second, prior studies have focused on a narrow set of outcomes (for example, mortality, diabetes and cardiovascular disease) ascertained at a single timepoint remote from the initial monitoring period. Our study used a hypothesis-generating phenome-wide association study approach, examining the association between step counts and the human phenome. In this manner, several new associations emerged including GERD, sleep apnea and MDD, which would likely go unidentified if disease phenotypes were selected a priori. Lastly, our analysis permitted incident disease to emerge at any point during clinical care rather than a prespecified follow-up time as performed in most cohort studies. One may speculate that this approach is more accurate with respect to the timing of incident disease and refines the temporal association between longitudinal activity and incident disease.
The findings of this study should be viewed in the context of several limitations. We were not able to account for daily step variations between different types of Fitbit models14 and seasonal differences15 as well as the occurrence of the COVID-19 pandemic because device data were not available at the time of analyses and data were date-shifted to protect privacy of participants. The characteristics of our study sample may limit the generalizability of our findings to more diverse populations. The majority of our cohort was relatively young, female, white and college-educated, and only included participants who owned Fitbit devices. Further, participants engaged in more steps per day (median 7,731 steps per day) than the average steps per day values reported for adults in the USA aged over 60 years16, suggesting that the analytical cohort in this study was more active. The fact that we were able to detect robust associations between steps and incident disease in this active sample suggests even stronger associations may exist in a more sedentary population. Therefore, further studies are needed including participants who are historically under-represented in biomedical research and those with activity levels that more closely mirror the general community.
Our data do not account for nonstepping activity such as swimming or cycling, such nonstepping movement is better captured via waveform or raw accelerometry and may provide additional insight into the association between physical activity and clinical diagnoses. Further, this study was observational in nature; therefore, causation should not be inferred. We acknowledge the potential for reverse causation in which the existence of a condition leads to taking fewer steps rather than the reverse. We attempted to mitigate this concern by focusing only on incident conditions and excluding any incident disease that emerged in the first 6 months of the monitoring period. Further, there is a potential for unmeasured confounding in our analyses because we were not able to account for an exhaustive list of potential confounders such as job status, environmental factors and differences in the usage patterns between participants over time17. Future studies are needed to investigate the impact of user behavior on health outcomes. Additionally, findings from exploratory logistic regression that did not find an association between steps per day and other outcomes such as cardiovascular diseases should be viewed with caution given that the analytical sample was relatively young, reported fewer outcomes and had limited follow-up. We excluded 15.4–16.0% (varies based on the outcome) of months due to fewer than 15 valid days of data in the Cox models. This missingness seems acceptable in comparison with prior studies which considered data to be valid if activity was captured on at least 3 out of 7 days (that is, up to 57% missing data)18. Lastly, we also acknowledge the limitations of using EHR data for outcomes ascertainment and the potential lack of specificity of diagnostic codes. It is possible that conditions are coded improperly, not coded at all or not recognized in the clinic. Nonetheless, our results reflect use of diagnostic codes in clinical practice across various medical systems, including large regional medical centers and federally qualified health centers.
Despite these limitations, the sources of data for our study are unique and offer an example of the potential clinical value of linking wearables data to the EHR. Published activity studies almost exclusively used research-grade actigraphs to measure steps and/or activity counts. In contrast, our data derive from commercially available devices. Although some fidelity is lost between research-grade and commercial devices, data from the latter are highly generalizable to a large portion of the public who own such devices. Activity data in this study date to the creation of a Fitbit account by the user. Therefore, the risk of an observer effect in this cohort is negligible because much of the activity data was collected before the participant consented to All of Us.
These findings may have important clinical and public health implications. We were unable to identify any published studies that investigated the association of physical activity data from a wearable device to health outcomes, defined using an individual’s EHR. Therefore, this study provides important new evidence that integration of these data sources is feasible and may provide valuable and actionable information for clinicians. Clinicians could monitor activity trends and provide evidence-based anticipatory guidance for activity tailored to an individual’s clinical characteristics and risk profile. For example, our data suggest that an individual with a BMI of 28 kg m–2 (can lower their risk of obesity 64% (95% CI 51, 80) by increasing steps from approximately 6,000 steps to 11,000 steps per day (Fig. 3). Although validation of these results is important, such data provide a necessary first step toward the development of personalized activity prescriptions. Further, wearables can also be used as an adjunct tool to encourage patients to engage in physical activity by allowing them to set, measure and track goals19. Finally, self-reported physical activity or exercise interventions may have potential beneficial effects to lower the incidence of depression20 and lower the severity of obstructive sleep apnea and associated comorbidities21. Therefore, these results provide support for the need for further research to examine the effect of real-world, unstructured physical activity to prevent or mitigate the effects of such conditions, including some previously unidentified activity-disease associations (for example, GERD).
In summary, using the data from AoURP, higher daily step counts were associated with reduced risk of several common, chronic diseases, including diabetes, hypertension, GERD, MDD, obesity and sleep apnea. This association between step counts over time and incident chronic diseases was consistent even after adjusting for potential covariates, including baseline steps per day and step intensity. Step intensity was also significantly associated with these incident diseases, although the relationships were less consistent than with step counts. These findings provide a new, robust source of evidence in support of the physical activity guidelines to prevent the risk of developing chronic diseases. If validated, these results may offer an evidence-base for refining activity recommendations based on an individual’s risk profile. This study also provides an example of the potential clinical value of linking data from commercially available wearables to the EHR.